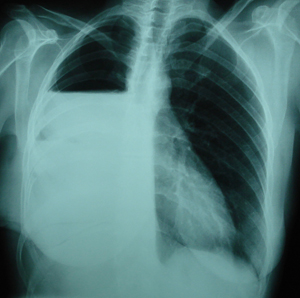
Figure 1
Postero-anterior chest X-ray. There is a large shadow at the right middle lung field. The mass seems to have smooth borders.

Figure 2
Chest CT scan, which shows a tumour mass, with smooth borders, located at the right middle lung field.
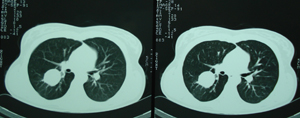
Figure 3
Postero-anterior chest X- ray, after a right thoracotomy and segmentectomy of the middle lobe. Twelve years postoperatively there is no sign of recurrence. Also the suture line throughout the lung parenchyma is visible.
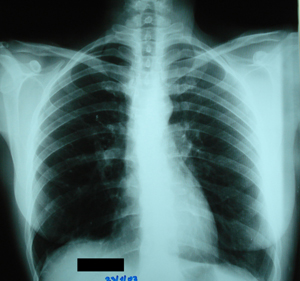
Figure 4
Postero-anterior chest X- ray, sixteen years after the segmentectomy shows a shadow close to the right hilum. Bronchoscopy, followed by biopsy confirmed the diagnosis of typical carcinoid of the lung.

Figure 5a
Chest CT scan, which shows nodular thickness of the parietal pleura of the right hemithorax. These findings are more compatible with metastatic lesions originating from the primary bronchial tumour.
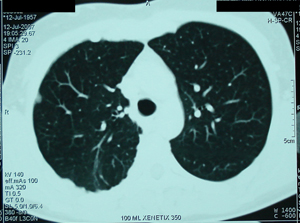
Figure 5b
Chest CT scan, at the level of the right hilum. A tumour mass is visible at the right hilum, which obstructs partially the intermedius bronchus.
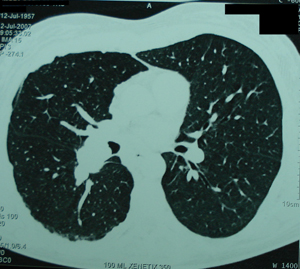
Figure 6a
Intraoperative photograph. After the mobilization of the parietal pleura. There are multiple nodules at the parietal and visceral pleura surface.
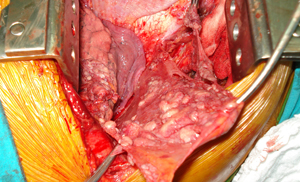
Figure 6b
Intraoperative photograph. There is a defect in the right hemidiaphragm, which has been resected en-block with the diaphragmatic parietal pleura. Also the upper surface of the liver is visible throughout the defect.
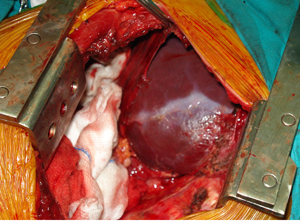
Figure 6c
Intraoperative photograph. Reconstruction of the diaphragm defect, with the insertion of a polu-tetra-fluoro-ethelene, synthetic graft, of 2 mm thickness, which was sutured continuously, using Prolene suture 1/0.
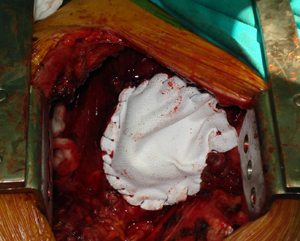
Figure 6d
Intraoperative photograph. After the pneumonectomy completion, the phrenic nerve is visible as well as many nodules that invade the pericardium.

Figure 6e
Intraoperative photograph. There is a defect in the pericardium and throughout this defect the myocardium of the right atrium as well as the right portion of the left atrium are visible.

Figure 6f
Intraoperative photograph. Reconstruction of the pericardium with the insertion of a Marlex-mesh synthetic graft. Also the synthetic graft of the diaphragm is visible.
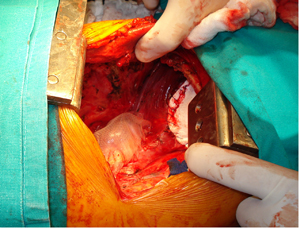
Figure 7a
Surgical specimen photograph, which shows the whole right lung, with the parietal pleura. There are many metastatic nodules scattered on the surface of the lung and the parietal pleura.
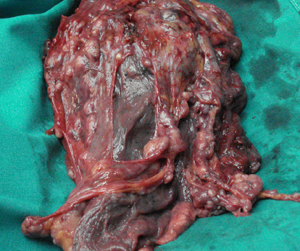
Figure 7b
Surgical specimen photograph, which shows the whole right lung and the resected parietal pleura. An incision over the primary tumour has been made.

Figure 7c
Surgical specimen photograph, which shows the resected diaphragm. There are few metastatic lesions.

Figure 7d
Surgical specimen photograph that shows the peritoneal surface of the resected diaphragm, without any abnormality.
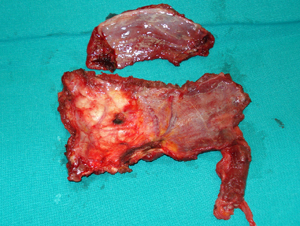
Figure 7e
Surgical specimen photograph, that shows the resected pericardium as well as the phrenic nerve.

Figure 8
Postero-anterior chest X-ray, thirty days postoperatively. Hyper-inflation of the remaining left lung, displacement of the mediastinal structures to the operative side, while an air-fluid level is evident in the right hemithorax, replacing the resected lung. Also the right hemidiaphragm is elevated. These radiological findings represent the expected image after a recent pneumonectomy.
Top