Case 1
Figure 1
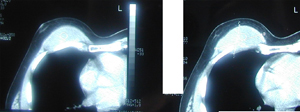
Chest CT Scan, which shows a large tumour of the chest wall with smooth borders, possibly originating from the muscles of the right hemithorax at the region of the mammary gland.
Case 1
Figure 2
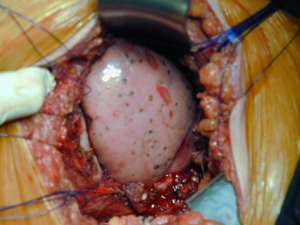
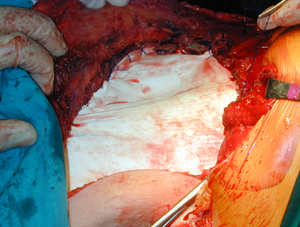
Intra-operative photograph. Chest wall defect after the resection of the chest wall tumour. The underlying lungs as well as the rib edges are visible. This case belongs to a young male patient.
Case 1
Figure 3
Surgical specimen photograph of the resected primary chest wall tumour. The histology examination revealed a desmoid chest wall tumour. It represents a very rare kind of chest wall tumours that may reccur even after a radical surgical resection.

Case 1
Figure 4
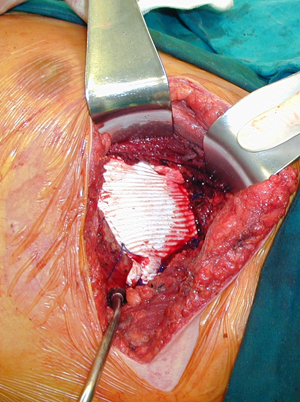
Chest wall reconstruction with the use of a synthetic graft (Poli-tetra-fluoro- ethelene).
Case 1
Figure 5
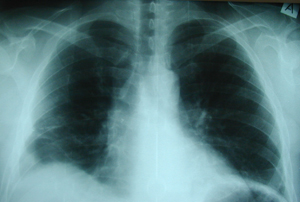
Postero-anterior chest X-ray that shows the edges of the right lower ribs after the resection of a chest wall tumour.
Case 2
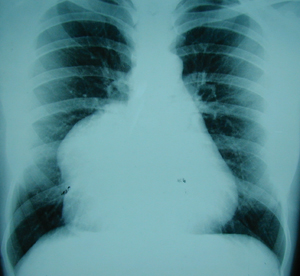
Figure 1
Postero-anterior chest X-ray, which shows a huge para-cardiac mass. This case belongs to a young female
patient.
Case 2
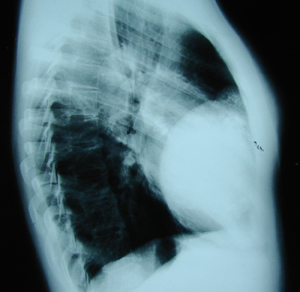
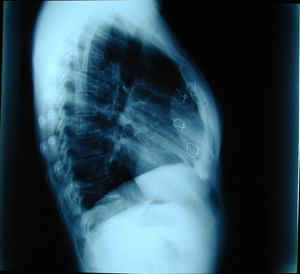
Figure 2
Lateral chest X-ray. A huge retrosternal mass at the lower third of the sternum, at the level of the xifoid process.
Case 2
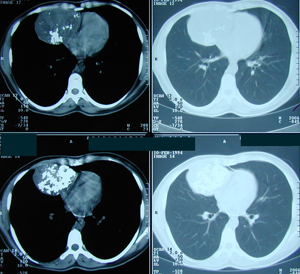
Figure 3
Chest CT scan which confirms the findings of the chest X-ray. It reveals a huge tumour mass of the chest wall originating from the lower part of the sternum and the anterior part of the 5th to 8th ribs.
Case 2
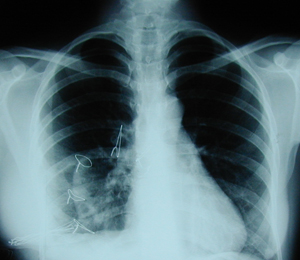
Figure 4
Postero-anterior chest X-ray after the excision of the tumour (chondrosarcoma), en block with the lower third of the sternum and the antero -lateral segment of the ribs. Chest wall reconstruction was achieved by the insertion of a synthetic graft of methy-Methacrylate (cement) with marlex- mesh graft. This technique is known as sandwich technique.
Case 2
Figure 5
Lateral chest X-ray after the resection of a primary chest wall tumour and the chest wall reconstruction.
Case 3
Figure 1
Chest CT scan. A huge tumour of the right lower part of the right chest wall. Also there is a pleural fluid accumulation, which causes atelectasis to the right lower lobe.

Case 3
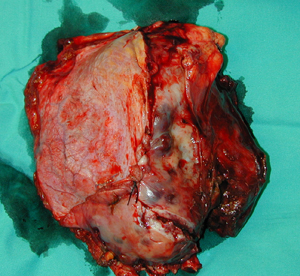
Figure 2
Surgical specimen photograph. The tumour was found to invade the right hemidiaphragm which was resected en-block with the anterior segment of the lower ribs (Costal arch). The histology examination showed a very rare metastatic tumour of the chest wall (Aesthesio-neuro-blastoma ), more than 25 years after the resection of the primary tumour.
Case 3
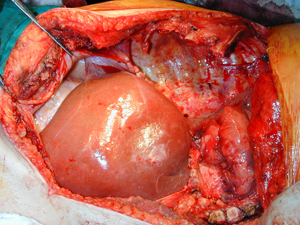
Figure 3
Intra-operative photograph. There is a defect in the chest wall and the diaphragm. The upper surface of the liver is visible.
Case 3
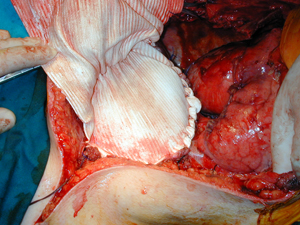
Figure 4
Intra-operative photograph. The diaphragm defect is reconstructed by the use of a synthetic graft (Poli-tetra-fluoro-ethelene), 2mm thickness.
Case 3
Figure 5
Intra-operative photograph. Chest wall reconstruction, ( replacement of the resected ribs ), by the use of the same synthetic graft.
Top